afib @ 90 bpm

First Glance:
Irregularly irregular predominantly narrow-complex rhythm at a reasonable rate.
Discussion:
First things first. The machine swears this is runs of VT, but this strip isn’t simple so the first plan of attack is make sure nothing scary is happening:
The rate looks reasonable and the complexes don’t look too wild. This is probably a perfusing rhythm. So we can take a deep breath and analyze casually..
This is irregularly irregular, which immediately brings atrial fibrillation to mind. Here’s another strip from the same patient:

All in all, the baseline has no consistent periodicity to it, so fibrillation fits. There are some sections of flutter-like baseline:

Here we can see some cyclic-appearing waves reminiscent of flutter at a rate of around 300. But these clean waves are clearly not tracking through the strip, and they aren’t regular, so this isn’t consistent with flutter. These larger P waves are probably just transient larger reentry loops in the atria before the smaller micro-reentry loops take back over.
What’s that orange triangle? It looks ventricular, so its either a PVC or an escape beat. Given we have one of the longer pauses before that beat, I’d lean towards escape. It would be unlikely to be a blocked beat because the ventricle has had plenty of time to repolarize before that unusual complex. More convincingly, we see an identical waveform as beat 4 of the first strip.
More interesting to me is the unusual-appearing wide complexes, especially in the first strip:
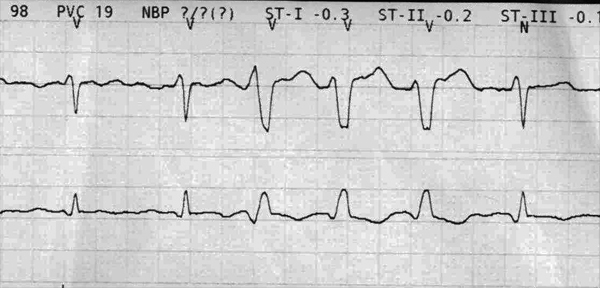
Here we see the narrow complexes apparently widening to a QRS complex with similar deflections but now with a QRS duration of up to ~130ms. These wide complexes look similar to an intermittent RBBB if we assume the V lead was slapped in the middle of the chest and is representing a septal lead.
The wide complexes look like they have 1-2mm of ST elevation (depending on where you look). Is this transient ischemia? I doubt it. I think we are seeing an intermittent conduction block below the AV node that is causing a brief nonspecific conduction delay. Some distal part of the conduction tree isn’t repolarizing fast enough, or isn’t conducting, so that little section of the ventricle conducts between myocytes resulting in a widening of the complex. Perhaps you already know that ST elevations that aren’t more than 5mm are rarely ischemic in LBBB? I think this is the same phenomenon. The aberrant beats have aberrant repolarization, thus the ST changes.
Do you trust the machine? The machine spat this out saying it was VT. It has marked the complexes for us with what it thinks are normal ‘N’ and ventricular ‘V’ complexes. But if you look through the strips it’s differentiation seems arbitrary. Not sure why- in a more straightfoward strip the machine is often able to accurately mark ventricular ectopy.
Final Impression?
Atrial fibrillation @ ~90 bpm with transient conduction delay and monomorphic PVCs.
Management implications:
No specific implications. Treat as afib. In a patient with more significant conduction disease than this, a transient block might require increased monitoring so as to avoid an unmonitored high-grade transient block with possible hemodynamic compromise.
The Take-home Point:
Conduction delays of any type can be transient. More commonly we can see a baseline conduction delay brought on by tachycardia and disappear after slowing of the rhythm or a ventricular pause (due to increased available time to repolarize slow ventricular conduction pathways), but that is not apparent here. These transient delays are often called ‘rate-dependent’ or ‘rate-related’ delays and can be tachy or bradycardia dependent.
Check out ECGpedia’s discussion of mechanisms of aberrant conduction, and note the diagrams on the right of that page.
![]() Three star strip. Devious stuff.
Three star strip. Devious stuff.