agonal rhythm
First Glance:
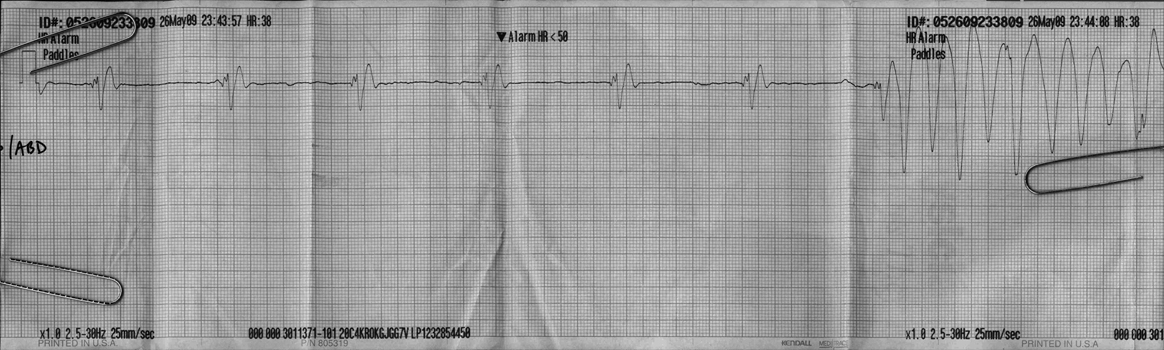
From across the room it looks like a bizarre bradycardia that converts to VT.
Discussion:
We are looking at the ‘paddles’ lead on a monitor, which is similar to lead I or II generally.
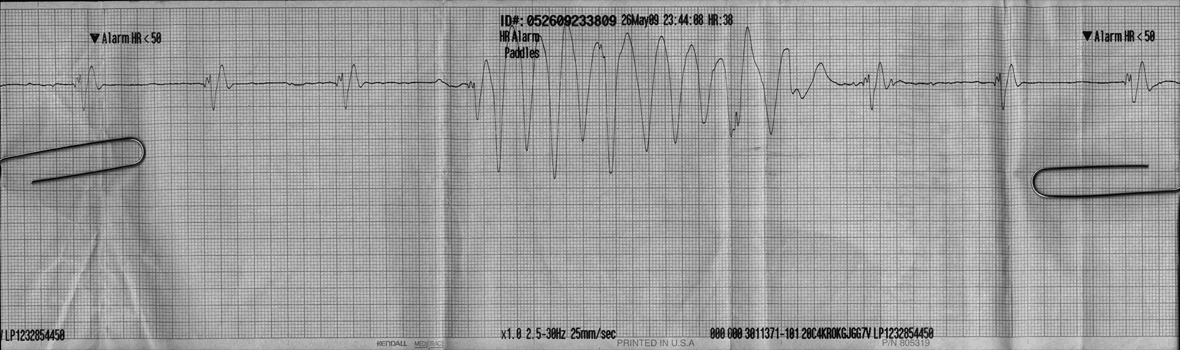
Here is the same strip, with a little more at the end:
First off, let’s look at the regular complexes that march across the first 3/4 of the strip. We see wide and bizarre complexes at 38 bpm, with no discernible atrial activity. These do not resemble any named named conduction abnormality. The wide bizarre complexes plus the bradycardia suggest strongly an agonal ventricular rhythm, or possibly an aberrant junctional rhythm. The amplitude of these QRS complexes (at standard gain) is far too large to represent atrial activity.
So what of the ‘VT’? You might think this was brief conversion to a shockable rhythm- superficially a good thing.
But it isn’t necessarily VT. It looks just like it, but we can see the squirrely initial bits of the weird complexes marching through this burst of activity (marked in pink below). You can’t have a regular ventricular QRS on top of a polymorphic ventricular tachycardia. Either this ‘VT’ is artifact, or the little squiggles that march through are atrial activity and there is AV dissociation.

AV dissociation is a lovely thing to see when differentiating wide complex tachycardias because it proves that the atria have nothing to do with the rhythm, thereby proving VT (and ruling out SVT with aberrancy). In this case it is not completely straightforward. The regular complexes have a couple sharp initial deflections (“squiggles”, which we can watch track through the ‘VT’). Those initial deflections are followed by a deep sharp S and a broader tall R.
The first part of the burst looks just like one of these complexes, but it is at the beginning of the burst and may not even be a part of the burst. The second squiggle superimposed over the burst looks like it is followed by a superimposed sharp S and a tall broader R, so this looks like it is tracking through. This would suggest that the burst of activity is either movement artifact (on some monitors CPR looks just like this- others have some filtering capability) or some electrical interference from any of the zillion devices on hand during a trauma code for a man shot in the chest five times (as this patient was). The third squiggle in the burst does not appear to have an obvious S and R, but this may have been erased by the excursive artifact’s waveform. Or it may be real. We have a dilemma.
A distant possibility is that those initial squiggles are actually retrograde P waves from a junctional escape rhythm. If this was VT, and the VT erased the ventricular component of the escape rhythm but the retrograde P waves were still conducting to the atria you could get AV dissociation with VT and the squiggles would march while the VT hammered away underneath. For this to be the case here, that second squiggle would have to have coincidental S and then R waves that just happened to look like the native agonal S and R.
So we are stuck. Either the burst is VT, because the third squiggle looks like AV dissociation and the second has coincidental deflections, or the burst is artifact, because the second squiggle looks like a marching QRS and the third has coincidental lack of deflections.
Final Impression?
Agonal bradycardia @ 38 bpm with a burst of polymorphic VT vs artifact.
Management implications:
An agonal rhythm is a bradycardic terminal rhythm. Fix the underlying etiology, but otherwise you are often dealing with a PEA arrest. In this particular strip, even if you thought this was VT you would be hard-pressed to shock the patient during the brief episodes.
A longer strip (with many more interpolated complexes) would definitively differentiate the rhythm, but unless that rhythm is sustained this is largely academic. There is no point shocking a brief paroxysmal rhythm nor an artifactual VT that is actually PEA.
The Take-home Point:
Wide and bizarre bradycardic complexes suggest agonal rhythm (or hyperkalemia).
![]() Two star strip. The meat and potatoes.
Two star strip. The meat and potatoes.