SVT with ectopy

First Glance:
From across the room it looks a regular narrow complex rhythm with a lot of ectopy and artifact.
Discussion:
We start with a regular supraventricular tachycardia @ ~ 150bpm which sees a PVC a little past halfway through, followed by more SVT but now at ~185 bpm. The change appears sudden, so we think about a PSVT. That would be consistent with a reentry loop that was initiated by the PVC.
Maybe in the first few beats you could pretend you see P waves, but the jury is still out if you only have this strip to go on.
There is some movement/loose lead artifact, and a few complexes which give this strip the look of polymorphic ventricular ectopy. However, if you march out the QRS complexes you see that they are all exactly on time with QRS-like deflections and the ventricular-appearing morphology is probably a little artifact superimposed on the native QRS. The machine says ‘multiform PVCs’, but if that’s the case it’s not from this strip. These aren’t likely fusion beats either because the on-time R wave is tight and matches the native R waves.
The exception is the beat below:
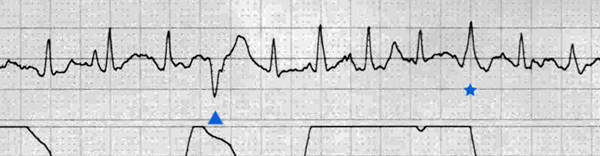
We see that off-sync PVC (triangle). Is the starred beat a fusion beat? I don’t think so. When the baseline is this fidgety you can imagine anything you want, but if it isn’t consistent, it probably isn’t worth calling.
Note the respiratory rate is fast.
Final Impression?
Regular SVT @ 150 bpm with one PVC, then conversion to 185 bpm suspicious for reentry.
Management implications:
This is fast- fast enough to be symptomatic in patients with cardiac disease. But sinus tach will be treated differently than reentry rhythms. Adenosine might be a good first shot if that 185 bpm rhythm is maintained because suspicion is high for a reentry tachycardia and even if it isn’t- the baseline might get quiet enough to pick out P waves. If you do this- do everything you can to minimize artifact and baseline jitters before pushing adenosine.
The Take-home Point:
PSVTs are often AV node reentry rhythms where a slow and fast pathway are allowed to form a loop by a PAC or PVC resetting the fast pathway so that the slow pathway is able to auto-cycle the loop.
PACs are the classic way to trigger AV nodal reentry tachycardia (AVNRT), which is more common. I read somewhere that a PVC as the instigating event might push you towards AVRT instead- ie: the slow pathway is through a bypass tract, instead of within the AV node.
![]() Two star strip. The meat and potatoes.
Two star strip. The meat and potatoes.