sinus rhythm with ectopy

First Glance:
From across the room it looks like sinus with some ectopy.
Discussion:
The upper lead is II and the lower is III. We can easily follow the P waves, the normal PR interval (~120 ms), and the QRS’s at an unremarkable 65 bpm until a premature supraventricular beat (beat 6) interrupts the cycle. Is it junctional or atrial ectopy?
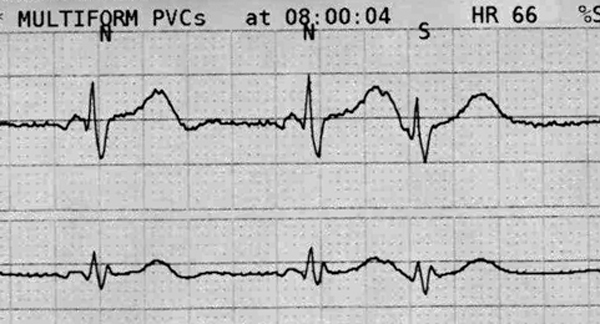
If you compare the T wave that follows each of the normal beats to the T wave that precedes the ectopic beat, we see it is slightly different: longer, with a subtle second positive deflection near the peak. This is a superimposed P wave, so this ectopic beat is a PAC.
At beat 8 we see the beginning of two couplets of ventricular bigeminy. You might have wondered for a second whether these are truly ventricular coupled beats, or whether they are just more PACs but now with aberrancy (that happens). However, close inspection shows no buried P waves before them, the T wave looks normal, and the interval is different. These are most likely what they look like from across the room- coupled PVCs.
These PVCs are followed by a ‘noncompensatory’ pause, which is a fancy and unintuitive way of saying that the sinus node was reset. We know that the sinus node was reset because if the sinus node had been unaffected by the PVC the atria would have likely been depolarized on time during the tail end of the PVC repolarization. We don’t see that, so the PVC depolarization was likely conducted into the atria resetting the sinus node.
The strip continues:

Just business as usual.
Does the QRS look unusual in III, the lower lead? As long as the QRS is not >120ms, the rsr’ morphology is not clinically significant there, and this is not an unusual finding in that lead.
The T wave looks biphasic in both leads, with a subtle deflection below baseline at it’s tail end. This could be a negative U wave, too, which is of unclear significance. U waves in general have soft significance, and the negative U wave is weakly suggested as indicative of cardiac pathology involving ischemia, volume overload, or coronary stenosis- a few examples are available in the literature if you google around a little.
One last strip- same patient, an hour later:

Here we see the same leads, but the rate has slowed, someone has decreased the gain on the lower lead from 60% to 30% (heck knows why), those negative U’s (vs biphasic T’s) have disappeared, and the P morphology in the upper trace now appears bifid (which on a standard 12L might be suspicious for LAE).
What caused all that? Who knows. We could make up all kind of weak theories- maybe the right atrial component of the earlier P in the upper trace was much larger due to volume overload. This made the first half (the right atrial half) of the P wave in that trace larger and obscured the bifid P at baseline. That volume overload could also have resulted in the negative U’s seen earlier and the ectopy.
That is clutching at straws for sure, but it’s an interesting exercise in hot-air physiology. Of note- I understand that P wave morphology can change just in the setting of rate changes, but they would not change this significantly. Further, P waves obviously change as you switch leads (if one electrode was moved), but this is less likely given how identical the before/after QRS complexes are.
Any other ideas?
Final Impression?
1) Normal sinus rhythm @ 65 bpm with atrial and ventricular ectopy.
2) Sinus bradycardia @ 50 bpm.
Management implications:
This is not a scary rhythm and a little ectopy is unlikely to significantly alter your patient’s cardiac output. However, new ectopy suggests some physiologic change and is worth a thought.
The Take-home Point:
Zillions of things cause ectopy including irritability secondary to ischemia, electrolyte disturbances (classically hypokalemia and hypercalcemia), wall stretch (volume overload), mechanical irritation (central lines, guidewires, or operative manipulation, etc), injury (infarction, contusion, etc), and pro-arrhythmic drugs.
![]() One star strip. Students should identify the rhythm correctly.
One star strip. Students should identify the rhythm correctly.