sinus tach with SVT

First Glance:
From across the room it looks like sinus tach with a run of faster regular narrow complex tachycardia
Discussion:
The original rhythm is presumably sinus tachycardia with diminutive P’s seen across the early strip with a flawless and regular baseline. Mid-strip we get a rhythm change:
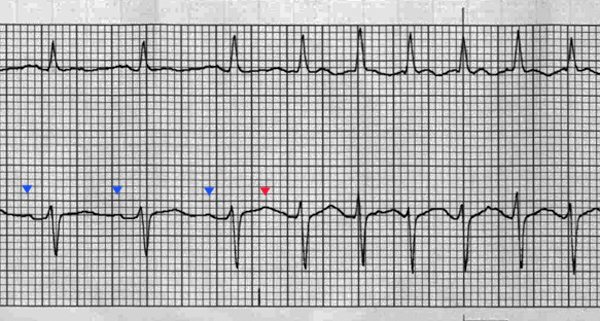
Here we see the onset of a faster regular tachycardia (now @ ~200 bpm) with identical QRS’s. So we know we have an SVT of some sort, but that doesn’t help differentiate between an irritable sinus node or a re-entry SVT or atrial tachycardia or whatever.
If we look at the start of this run, we can pick out the sinus P’s (dark purple) with regular QRS’s followed by identical T’s. Then, suddenly the T wave is a little bit different after one beat (magenta triangle) and the new rhythm starts. I’d suggest that this unusual T might be a native T plus an ectopic atrial beat which allows a re-entry circuit to activate in the AV node.
The ST segments within the run are also with different morphology than before, allowing the possibility of some superimposed retrograde P waves. This is a stretch to call from these strips, however.
Here’s another strip from the same guy:

Here we start with sinus @ ~115 bpm, then see what looks like a PAC at beat 12 (P wave before QRS with normal PR interval but new morphology), followed by a regular rhythm somewhat faster at ~150 bpm with P waves with different morphology but still normal PR interval.
See the early P waves in the upper lead? They look wide, positive, and bifid. After the rate change they are hard to pick out of the baseline. In the lower lead they begin positive, and after the rate change they appear more subtle, but seemingly negative.
That sounds like an atrial tachycardia, where the AV node is being paced by an ectopic atrial focus. Does that change my mind about the first strip? Not really, but if we are having atrial ectopy that makes me think more along the lines of PSVT secondary to PACs or another atrial tachycardia is more likely than the sinus node just up and speeding up.
Anything else we can say? That unusual P morphology in the first half of lead II?
We have bifid P’s (with peak to peak distance of 40ms or greater), and they are on the long side, so I’d check the 12L or echo for evidence of left atrial enlargement.
Final Impression?
1st strip: ST with PSVT vs AT
2nd strip: ST then AT
Management implications:
If this is atrial tachycardia, efforts to identify any pro-arrhythmic or pro-atrial-irritant effects should be made. Digoxin, hypokalemia, caffeine, and sympathomimetics might do this. These rhythms are generally perfusing as they still have atrial contractions followed by ventricular contractions, but if the rate gets too high you will treat acutely hemodynamically unstable patients per usual (shock vs medicate, adenosine is less likely to work than with AV re-entry tachycardias) and chronic atrial tachycardia patients with various EP procedures.
The Take-home Point:
If the P wave axis is abnormal, it isn’t sinus-paced.
![]() Three star strip. Devious stuff.
Three star strip. Devious stuff.