sinus rhythm with ectopy

First Glance:
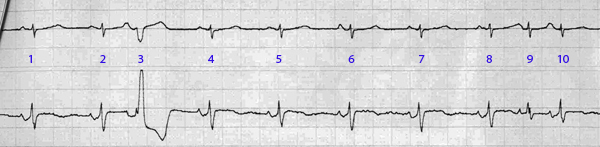
From across the room it looks like a regular narrow complex rhythm with multifocal ectopy.
Discussion:
The underlying rhythm is clearly sinus. We see regular narrow complex QRS complexes marching across both lead II and the chest lead, with P waves with normal morphology in II (positive) and presumably septal (biphasic: positive then negative) respectively.
We also see six premature beats. Three are wide and PVC-like. Three are narrow. Let’s start from the beginning:
Beat 1 and 2 are sinus. Beat 3 is wide and early. I would normally think this was a PVC but if you look before this bizarre QRS complex you see that the prior T wave was abnormal. In fact, all the sinus beats have identical T waves across this strip except the ones followed by ectopy. In a strip with a clean baseline like this one, this suggests that those are normal sinus T waves with superimposed premature atrial depolarizations. So beat 3 is an aberrantly-conducted PAC, not a PVC. Maybe the conduction pathways had not completely repolarized yet, so part or most of the purkinje fibers do not fire, so the depolarization wave sloshes slowly across the ventricular myocardium and gives you the QRS morphology that looks exactly like a PVC- but it isn’t.
If we note that the chest lead is septal, the positive axis in V suggests a rate-dependent RBBB which is consistent with the aberrant septal rsR’ morphology in the wide beat.
Beats 4-8 are sinus. 9 is a PAC, but this time conduction is normal, and you get another weird T wave followed by a premature beat, but this time with a narrow/supraventricular complex. Classic PAC. It is followed quickly afterwards by another narrow beat (10). This is a sinus beat again. It is exactly the same spacing and morphology as the other sinus beats. It’s P wave looks a little spiky because it is a sinus P on top of the T wave from the premature beat. That means this PAC was followed by a ‘compensatory’ pause.

Beats 10 to 12 are sinus. 13 is another PAC. But this time 14 looks like a PAC too, because it’s P wave is a little different than the sinus P waves, and because it does not appear to be on time for either a sinus P after a compensatory pause, nor after a non-compensatory pause.
A normal-length pause follows, and the next beat (15) is sinus. 16 is another aberrant PAC, then there is another sinus/aberrant PAC couplet, then 19 and on is sinus.
Final Impression?
Sinus rhythm @ ~80 bpm, with frequent premature atrial ectopy with intermittent aberrant conduction.
Management implications:
This is a lot of atrial ectopy, and there was a couplet. We can’t say definitively whether this is all coming from the same focus, but it could well be some irritable focus in one of the atria. Do they have a central line that is in too deep (and is tickling the atria)? That could do this.
If this person breaks into a sustained tachycardia, you would have a high suspicion for ectopic atrial tachycardia.
The Take-home Point:
Sometimes folks make reference to an ectopic beat causing a ‘compensatory’ or ‘noncompensatory’ pause, which indicate whether the sinus node has been reset.
What does it tell you if an ectopic beat is noncompensatory? It means it resets the sinus node, starting the cycle over as the atria is depolarized retrograde.
In my very limited experience differentiating the type of pause after an ectopic beat has limited clinical value at the bedside, but it makes you sound like you know what you’re talking about- even if you don’t. That could be a bad thing.
![]() Two star strip. The meat and potatoes.
Two star strip. The meat and potatoes.
This is a 3-STAR strip (not 2 stars as given) in my opinion. I agree that the rhythm is sinus with frequent PACs. P wave morphology does vary – so more than one atrial focus. That puts this rhythm somewhere along the spectrum of between sinus rhythm with PACs vs MAT (closer to the former – but with similar implications as if it were the latter).
As you correctly indicate – many of the PACs occur with aberration. This is not “rate-related aberration” which is something else – but rather a function of PACs arriving at the ventricles at a moment when part (not all) of the ventricular conduction system has recovered.
The widest PACs conduct with a bifascicular block pattern of aberrancy (RBBB/LAHB) – as diagnosed by rsR’ in MCL-1 and predominantly QRS in lead II. Aberrancy typically conducts with some pattern of BBB. In general – the refractory period of the right bundle branch is longest – so the most common form of aberration is with RBBB morphology (that may occur with or without a hemiblock).
I prefer not to use the term “compensatory pause” in association with PACs – because by definition with a PAC you are ALWAYS resetting the SA node … Rather than the interval between #8-to-10 reflecting a compensatory pause – I think we just have 2 PACs in a row …. Although I always look for “full compensatory pauses” with PVCs – I agree with you that this sign in general has limited diagnostic value. Of much greater value is following along with your calipers to see if any atrial activity that you see is right on time or not ….
Very interesting. I had imagined that what you describe was effectively rate-related aberrancy given the faster the rate, the less likely the full conduction system was likely to be completely repolarized.
an interesting and relevant article here, for folks interested in rate dependent aberrancy: http://circ.ahajournals.org/content/48/4/714.full.pdf+html
I had imagined (based on theory, not clinical experience) that you could get true compensatory pauses with PACs if there were atrial conduction defects as seen in sinoatrial exit block, etc. Obviously the expected result of an atrial depolarization is sinus reset, but interpolated PACs would suggest the ability of unusual PACs to depolarize the atria without resetting the SA node. But I agree your explanation makes much more sense than my zebra!