sinus rhythm
First Glance:
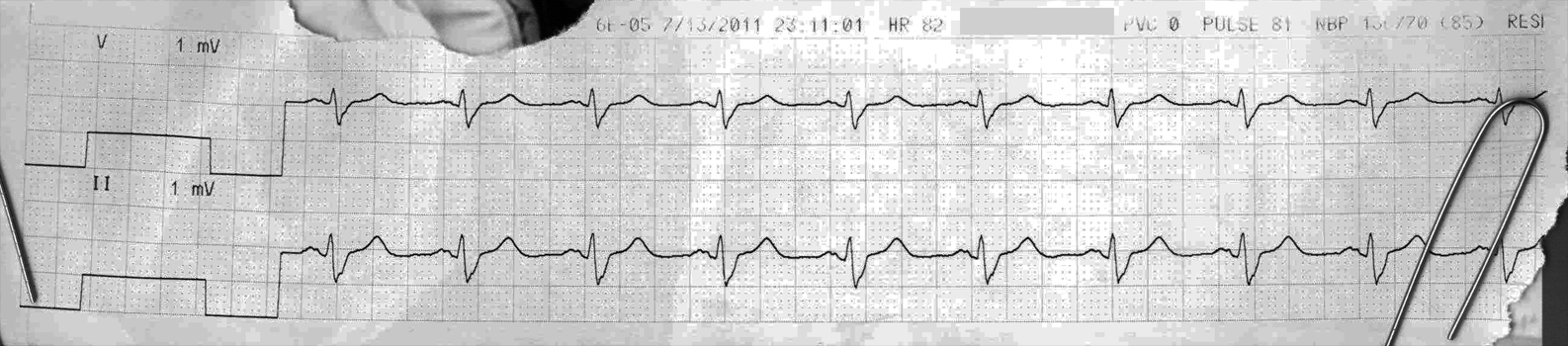
From across the room it looks like a wide complex sinus rhythm.
Discussion:
This will be a quick one.
We easily see lovely P waves before each QRS in this regular rhythm. The P wave axis is normal in II (lower lead) so this is presumably sinus. The P waves are bifid with about 40ms between peaks, so the hypersensitive amongst us might wonder about LAE. However, tele strips don’t have good precision in terms of deflections heights so we can’t make that call.
The complexes are wide, about 130 ms wide, so we have some kind of conduction system pathology. Here we see a deep S in II. This looks a bit like it might in RBBB or in high-lateral LBBB (when the big monophasic R waves are in I and AVL, as opposed to V5 and 6), but this is a stretch and will need perusing other leads to explore.
Final Impression?
Sinus rhythm @ ~80 bpm, suspicious for BBB.
Management implications:
Check old QRS and P morphology. New QRS widening is clinically significant. 12L to evaluate properly. Ask patient about cardiac symptoms, etc.
The Take-home Point:
Any new conduction aberrancy (RBBB or LBBB or a fascicular block or a nonspecific conduction abnormality) could be ischemic dysfunction of some part of the conduction system. A new LBBB is particularly commanding because it is a STEMI equivalent. That is to say, new or presumed-new LBBB is the same thing clinically as ST elevation. And you know how excited we get about that, right?
![]() One star strip. Students should identify the rhythm correctly.
One star strip. Students should identify the rhythm correctly.
This is normal sinus rhythm – as defined by the presence of an upright P wave with fixed and normal PR interval in lead II. The QRS is wide.
It is best NOT to overcall atrial morphology on a rhythm strip. The ECG is notoriously in its poor sensitivity and poor specificity for atrial enlargement. Moreover – sometimes there may be internal magnifications in amplitude on rhythm strips – such that you should NOT call any atrial abnormality (in my opinion) on the basis of what you see on a rhythm strip – with possible exception of increased suspicion for RAE if you truly see very tall (>3-4mm) peaked “uncomfortable to sit on” P waves in lead II.
The wide QRS with sinus rhythm indicates some type of conduction defection. You cannot diagnose LBBB on what we see. This is highly unlikely to be aberrancy. BEST not to say (speculate) anything more than what we know = sinus rhythm with QRS widening presumably from some type of conduction defect. A 12-lead is needed to say any more.
Thanks for the comments!
I think you mean, “highly unlikely to be LBBB”?
Point taken. thanks again-