whoa. what is that?

First Glance:
From across the room it looks crazy- something like bigeminy over an atrial tachycardia?
Discussion:
This strip intimidates the heck out of me.
The most visually commanding thing in this strip is the sharp fast-paced apparent tachycardia most obvious in the chest lead. It hovers around 250-300 bpm, and is quite irregular in places.
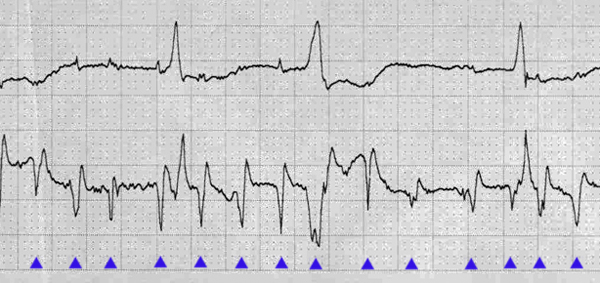
The morphology is unlike what we expect in atrial flutter. For the irregularity and the morphology I lean away from atrial flutter, but I do believe it’s atrial because there is a distinct ventricular rhythm seen in the upper lead.
Author’s note: Expert review concludes this is artifact. Read further for a discussion of one way to pick apart the strip, but see excellent comments at the bottom of the page for the definitive read.
Lets look at lead II. Here we can see larger complexes with an irregular rhythm- alternating narrow and wide beats. It actually looks like ventricular bigeminy, but these are not actually regular couplets. The first ‘couplet’ has an RR interval of about 1020 ms. Then the RR intervals continue: 820, 720, 720, 710, 680. The wide beat could be a ventricular beat, a fusion beat, or it could be an aberrant supraventricular beat- maybe with intermittent or rate-dependent LBBB as this is lead II.
Usually when I see a raging baseline like this I assume there is probably a fast atrial rate with AV block. Here that is less likely because there is no consistent interval between the fast baseline and the ventricular complexes. Maybe this is a junctional escape rhythm with ventricular bigeminy, some unusual atrial tachycardia, and a complete heart block. I just don’t know, and the patient is long gone for any kind of clinical correlation. I don’t think the fast baseline is artifact, because it has an ‘electrical look’ to it, and it’s irregular. Electronic and bed vibration artifact is usually mechanically regular. Tremor artifact is not, but does not result in these very sharp deflections in my experience.
Final Impression?
Unknown rhythm with ventricular rate of ~65 bpm. Post up if you can break this open for us.
Management implications:
We can’t make management suggestions if we have no idea what we’re working with. Checking leads on the patient, other leads, a 12L, and old strips or 12L will show us the way.
The Take-home Point:
You can’t make a definitive diagnosis in many cases from a tele strip.
![]() Three star strip. Devious stuff.
Three star strip. Devious stuff.
Unfortunately since you don’t have clinical correlation on this one – we will never know …. (which is nice, because it means I can speculate anything and not be “wrong”). That said – I think the overly rapid and irregular spikes (best seen on the lwoer tracing) represents ARTIFACT. The baseline is terribly erratic – morphology does have an “electric feel” to me given its general verticality – and it just doesn’t make sense to have something so fast and irregular … Clinically in cases like this – the 1st thing I do is look at the patient (and that usually gives me the answer in the form of shivering, scratching, tremor, etc.).
The ventricular rhythm in the top tracing looks real however – and it is quite interesting. As you note the coupling interval of the seemingly “bigeminal” rhythm varies – so it is NOT simply bigeminy. Moreover – the coupling interval is clearly longer than is usually seen with “PVCs”. There is NO reason for these relatively late occurring beats to conduct with aberration – so that is NOT an explanation. Wide beats with varying coupling raises the question of parasystole – but with all the artifact that I see (as well as other “nonfollowers”) – I’m not prepared to hazard any guess without some clinical correlation and a better quality tracing. I agree with your last sentence: “You can’t make a definitive diagnosis in all cases from a tele strip”.
Points well taken. Thanks for your excellent commentary!