ST elevation

First Glance:
From across the room it looks like tachycardia with ST elevations.
Discussion:
It’s a regular narrow complex rhythm at a little under 100. There is clearly ST elevation. I can see little positive deflections at the end of the inverted T wave that would be unusual for a T wave, so I feel confident that it is a P wave here (blue triangles, below). I wouldn’t be surprised if this met criteria for first degree block in other leads, but we can’t make that call from this lead.
When I look at leads like this I sometimes wonder where the QRS ends and the ST segment begins. After all, how will I know where to measure to to decide if this is a wide complex?
The standard answer is to measure to the J point. The J point is where the trace ‘turns a corner’. Look at the last beat below and see where the QRS is rising out of the deep S wave and there is a place about 1mm above the baseline where it makes a subtle angle and reduces its slope? That is the J point. I marked two with red dots below.
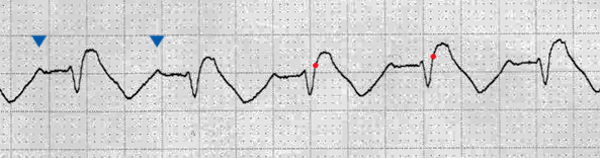
Here the QRS is narrow because the rS complex is less than 120 ms from the beginning of the R to the J point, and the ST elevation is ~2mm because it is 3mm from peak to baseline at a gain of 140%. Importantly, the ST segment elevation is convex-up (dome-like), a morphology consistent with myocardial injury.
Final Impression?
Sinus rhythm @ ~95 bpm with 2mm ST elevation and T inversion in MCL concerning for injury.
Management implications:
12L for evaluation of ischemia/infarction/AV delay. Check which lead MCL is used here and compare with old EKG to see if there is morphology change.
The Take-home Point:
‘MCL’ is the Modified Chest Lead. It can be slapped anywhere on the chest, so just because it says ‘MCL’ on the monitor doesn’t mean you know what the QRS morphology should be. It is generally used to give a V lead (chest lead) view using limited leads. In my experience it is generally slapped on the sternum which gives a septal view, but you can’t be sure without looking.
With a 5-lead telemetry box, with four limb leads and one chest lead, you can have simultaneous recording of all limb leads plus one chest lead. Which chest lead you gets depends on where you put the chest lead, and that chest lead is exactly the same as the standard V-lead who’s place it occupies. Ie: if you put the chest lead of a 5-lead tele box in the V3 position, you will get the same V3 readout that you would get on a 12L EKG. The negative electrode is the average of the three active limb leads (RL is ground). The positive lead is the chest lead. This is how a 12L works.
With 3 leads or less you can’t get a ‘true’ V-lead because you need three leads alone to calculate that ‘average’ of the active limb leads. However, we still want chest leads because they give us great information about atrial activity and anterior regions of the myocardium. Therefore, the poor man’s chest lead with a 3-lead EKG is MCL. It uses LA as the negative electrode and a chest lead as the positive electrode. Technically the terminology is such that MCL1 is when the MCL lead is placed in the V1 position, MCL2 is V2 position, etc. MCL leads give morphology similar to the corresponding V-lead, but not always exactly, and it’s hard to predict how similar they are. However, it’s pretty darn good, and generally you can get everything you need for monitoring purposes. As always, we confirm all findings with the official 12L.
![]() One star strip. Students should identify the rhythm correctly.
One star strip. Students should identify the rhythm correctly.